
Custom Search
Molar pregnancy....snow white appearance on ultrasound
Molar pregnancies are an uncommon and very frightening complication of pregnancy and occurs due to an abnormal fertilization process.The formal medical term for a molar pregnancy is "hydatidiform mole."
The diagnosis of molar pregnancy can nearly always be made by ultrasound, because the chorionic villi of a typical complete mole proliferate with vacuolar swelling and produce a characteristic vesicular sonographic pattern.
• Previously when the diagnosis was made at a later stage, the classical ‘snowstorm’ pattern of the uterus was described; however this is not commonly seen now.

sonographic appearance of a complex and echogenic intrauterine mass containing many small
cystic spaces {which correspond to the hydropic villi on gross pathology}.
The diagnosis of molar pregnancy can nearly always be made by ultrasound, because the chorionic villi of a typical complete mole proliferate with vacuolar swelling and produce a characteristic vesicular sonographic pattern.
• Previously when the diagnosis was made at a later stage, the classical ‘snowstorm’ pattern of the uterus was described; however this is not commonly seen now.

Scan of the uterus shows the classical bunch-of-grapes appearance or snow-storm appearance in the uterine cavity is noted. This is the typical appearance of a gestational trophoblastic disease.
• Benson et al reported that the majority of first trimester complete moles demonstrated a typicalsonographic appearance of a complex and echogenic intrauterine mass containing many small
cystic spaces {which correspond to the hydropic villi on gross pathology}.
X-ray Osgood-Schlatter disease
Osgood Schlatters disease is a very common cause of knee pain in children and young athletes usually between the ages of 10 and 15. It occurs due to a period of rapid growth, combined with a high level of sporting activity.
* Normal x-ray findings do not exclude the disease, which is diagnosed clinically
* Radiographs have Limited role "Clinical diagnosis"...............

Imaging Findings
* Normal x-ray findings do not exclude the disease, which is diagnosed clinically
* Radiographs have Limited role "Clinical diagnosis"...............
Lateral radiograph of the knee demonstrating fragmentation of the tibial tubercle with overlying soft tissue swelling.
Hallux varus in X-ray

The condition has various degrees ..............

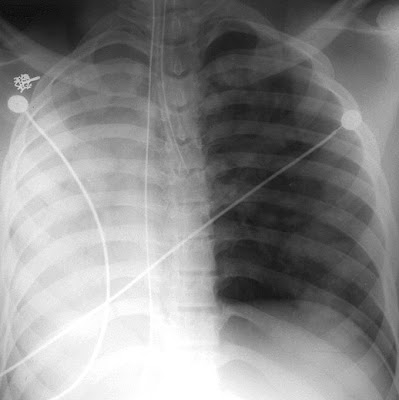
Acute pulmonary edema following surgery

- a. Left lower lobe pneumonia.
- b. Acute pulmonary edema.
- c. A large pneumothorax.
- d. A large pericardial effusion.
- e. A ruptured gastric ulcer.
Correct Answer: Acute pulmonary edema.
Explanation
There is diffuse airspace disease in both lungs causing almost complete opacification of both lungs. This came on suddenly and is characteristic of pulmonary edema. Other fluids can inhabit the airspaces such as blood or gastric aspirate, but they have different clinical stories and are less common than acute pulmonary edema. This patient had been hypotensive and was suffering from non-cardiogenic pulmonary edema. Vasopressors and diuretics were used in his treatment.
Scaphoid fractures overview

Anatomic snuffbox tenderness is a highly sensitive test for scaphoid fracture, whereas scaphoid compression pain and tenderness of the scaphoid tubercle tend to be more specific. Initial radiographs in patients suspected of having a scaphoid fracture should include anteroposterior, lateral, oblique, and scaphoid wrist views..........
READ MORE................>>

Congenital aortic stenosis in X-ray
In Supravalvular aortic stenosis you can see Aortic knob is often small due to underdevelopment and stenosis of the supravalvular portion of the aorta. Different from the poststenotic aortic dilation that occurs with valvular aortic stenosis.


Congenital aortic stenosis. Small aortic arch with moderate enlargement of the left ventricle.
Indications of Thumbprint sign in Chest & Abdominal X-ray

the thumbprint sign is a finding on a lateral C-spine radiograph that suggests the diagnosis of epiglottitis. The sign is caused by a thickened free edge of the epiglottis, which causes it to appear more radiopaque than normal, resembling the distal thumb.

Thumb’ like epiglottitis. Note the swollen epiglottitis like a thumbprint
" enlarged epiglottis in epiglottitis which, instead of its usual thin fingerlike projection, is stubby, like the thumb "
In an abdominal x-ray, the "thumb print sign" has similar appearance of thumbs protruding into the intestinal lumen, but are in fact caused by thickened edematous mucosal folds. Abdominal thumbprinting a sign of intestinal ischemia.

Pericardial Effusion Vs Pleural Effusion
Usually pericardial effusion(PE) is not found behind the left atrium,because the pericardial attachments are refleted onto the pulmonary veins.Somtimes,PE can be visualized in the oblique sinus,which is located behind the LA. A PE is anterior to the descending aorta,whereas a pleural effusion(PL) is posterior to the aorta.
What are Occipito-mental Views ? And lines for inspection.
(click on images to enlarge)

Occipito-mental View
The PA occipito-mental view provides excellent demonstration of the upper and middle thirds of the face including the orbital margins, frontal sinuses, zygomatic arches and maxillary antra.

Occipito-mental 30 View :
With 30 degrees of caudal angulation, the orbits are demonstrated less well. However, the zygomatic arches and the walls of the maxillary antra are seen clearly.
There are 3 lines for inspecting the OM views:


Line 1:
Look for widening of the zygomatico-frontal suturesFractures of the superior rim of the orbits
“Black-Eyebrow” sign due to orbital emphysema
Opacification / air-fluid level in the frontal sinuses
Line 2:
Look for fractures of the superior aspect of the zygomatic archFractures of the inferior rim of the orbits
Soft tissue shadow in the superior maxillary antrum
Fractures of the nasoethmoid bones and medial orbits
Line 3:
Look for fractures of the inferior aspect of the zygomatic archFractures of the lateral maxillary antrum
Opacification / air-fluid level in the maxillary sinuses
Fractures of the alveolar ridge
Compare the injured side with the uninjured side.
Noncontrast helical CT is the most sensitive and specific for the detection of renal stones
Which of the following tests is the most sensitive and specific for the detection of renal stones?
This imaging modality is fast and accurate, and it readily identifies all stone types in all locations. Its sensitivity (95% to 100%) and specificity (94% to 96%) suggest that it may definitively exclude stones in patients with abdominal pain.

- A) KUB plain film
- B) Ultrasound
- C) Intravenous pyelography
- D) Noncontrast helical CT
The answer is D.
Compared with abdominal ultrasonography and KUB radiography, intravenous pyelography has greater sensitivity (64% to 87%) and specificity (92% to 94%) for the detection of renal calculi. Noncontrast helical CT is being used increasingly in the initial assessment of renal colic.This imaging modality is fast and accurate, and it readily identifies all stone types in all locations. Its sensitivity (95% to 100%) and specificity (94% to 96%) suggest that it may definitively exclude stones in patients with abdominal pain.

Multiple transverse nonenhanced CT images demonstrate numerous 3-5-mm renal calculi (arrows) that were not depicted at US.
Ultrasound image of a normal eye with lens
Since the eye is a fluid-filled structure, it provides a perfect acoustic window, producing images with excellent detail. The normal eye appears as a circular hypoechoic structure. The cornea is seen as a thin hypoechoic layer parallel to the eyelid.
The anterior chamber is filled with anechoic fluid and is bordered by the cornea, iris and anterior reflection of the lens capsule. The iris and ciliary body are seen as echogenic linear structures extending from the peripheral globe towards lens. The normal lens is anechoic. The normal vitreous chamber is filled with anechoic fluid. Vitreous is relatively echolucent in a young healthy eye.
Sonographically, the normal retina cannot be differentiated from the other choroidal layers. The evaluation of the retrobulbar area includes optic nerve, extraocular muscles and bony orbit. The optic nerve is visible posteriorly as a hypoechoic linear region radiating away from globe.

Ultrasound image of a normal eye with lens
The anterior chamber is filled with anechoic fluid and is bordered by the cornea, iris and anterior reflection of the lens capsule. The iris and ciliary body are seen as echogenic linear structures extending from the peripheral globe towards lens. The normal lens is anechoic. The normal vitreous chamber is filled with anechoic fluid. Vitreous is relatively echolucent in a young healthy eye.
Sonographically, the normal retina cannot be differentiated from the other choroidal layers. The evaluation of the retrobulbar area includes optic nerve, extraocular muscles and bony orbit. The optic nerve is visible posteriorly as a hypoechoic linear region radiating away from globe.

Normal ocular ultrasound
Recurrent Pyogenic Cholangitis (RPC)

Recurrent pyogenic cholangitis,Cholangiohepatitis, is an uncommon disease in the western world Most of these cases are seen in Asian countries.
The etiology is unknown, although some of these patients have biliary parasites.
The disease is characterized by a recurrent syndrome of bacterial cholangitis that occurs in association with intrahepatic pigment stones and intrahepatic biliary obstruction.
-These patients are also at risk of developing biliary cirrhosis and cholangiocarcinoma.
-The left lobe is the most common location of the disease due to the delayed drainage of the left system.

This C.T. image shows a typical case of Recurrent pyogenic cholangitis
There is focal dilatation of the bile ducts in the left lobe with stones.
Below there is another example of recurrent pyogenic cholangitis.There is intrahepatic lithiasis with focal diatation.
A case like this is indistinguishable from focal Caroli disease with secundary stone formation.

Causes of lung collapse
Lung collapse usually occurs due to proximal occlusion of a bronchus, causing a loss of aeration. The remaining air is gradually absorbed, and the lung loses volume.
There are many causes for collapse, the most frequent are listed below:
* The commonest cause is a proximal stenosing bronchogenic carcinoma, which occludes a bronchus. Patients are middle aged or elderly, and almost always smokers.
* In a young adult or older child asthma is by far the commonest cause. Collapse occurs secondary to mucous plugging of the major airways, and responds to physiotherapy.
* In an infant consider an inhaled foreign body, such as a peanut.
* Retention of secretions is a frequent cause of post operative collapse.
* In ventilated patients, including neonates, collapse may occur if the endotracheal tube is inserted too far, entering one main bronchus and occluding the other as shown below:
There are many causes for collapse, the most frequent are listed below:
* The commonest cause is a proximal stenosing bronchogenic carcinoma, which occludes a bronchus. Patients are middle aged or elderly, and almost always smokers.
* In a young adult or older child asthma is by far the commonest cause. Collapse occurs secondary to mucous plugging of the major airways, and responds to physiotherapy.
* In an infant consider an inhaled foreign body, such as a peanut.
* Retention of secretions is a frequent cause of post operative collapse.
* In ventilated patients, including neonates, collapse may occur if the endotracheal tube is inserted too far, entering one main bronchus and occluding the other as shown below:

Complete collapse of the right lung in this case was caused by an endotracheal tube that was advanced too far and entered the left mainstem bronchus. The heart is not seen as the mediastinum is shifted to the right. There is overinflation of the left lung, also contributing to the mediastinal shift.
Ultrasound showing Bilateral communicating hydrocele in neonate
The below ultrasound images show gross bilateral communicating hydrocele in a neonate, which was found to have Hydrops fetalis in utero. Note the presence of ascitic fluid with communication with the hydrocele (arrow in last figure below).






Benefits of Schüller view on showing Mastoid bone
Schüller's view (Runstrom) is a lateral view of the mastoid obtained with the sagittal
plane of the skull parallel to the film and with a 30° cephalocaudal angulation of the x-ray beam.
These 30° in Schüller's view displaces the arcuate eminence of the petrous bone downward and shows the antrum and the upper part of the attic.
Schüller's view also gives an excellent view of the extent of the pneumatization of the mastoid,the distribution and the degree of aeration of the air cells, the status of the trabecular pattern, and the position of the vertical portion of the lateral sinus.

plane of the skull parallel to the film and with a 30° cephalocaudal angulation of the x-ray beam.
These 30° in Schüller's view displaces the arcuate eminence of the petrous bone downward and shows the antrum and the upper part of the attic.
Schüller's view also gives an excellent view of the extent of the pneumatization of the mastoid,the distribution and the degree of aeration of the air cells, the status of the trabecular pattern, and the position of the vertical portion of the lateral sinus.

Schüller view: Well-developed normally pneumatized mastoidal air cells can be observed in the picture on the left side (double arrow). In the picture on the right side, the mastoid cells (arrow) are obscured, and not air-containing, due to chronic otitis media.
Characteristic black pleura sign in Alveolar microlithiasis in chest X-ray
Alveolar microlithiasis is a rare disease of unknown etiology characterized by the presence of a myriad of very fine micronodules of calcific density in the alveoli of the lungs of a usually asymptomatic person. Characteristic black pleura sign (due to contrast between the extreme density of the lung parenchyma on one side of the pleura and the ribs on the other side).
Alveolar microlithiasis appears in Chest X-ray as diffuse, very fine micronodules of calcific density that are usually asymptomatic. Characteristic black pleura sign (it is due to contrast between the extreme density of the lung parenchyma on one side of the pleura and the ribs on the other side).

Alveolar microlithiasis appears in Chest X-ray as diffuse, very fine micronodules of calcific density that are usually asymptomatic. Characteristic black pleura sign (it is due to contrast between the extreme density of the lung parenchyma on one side of the pleura and the ribs on the other side).

Alveolar microlithiasis. Nearly uniform distribution of typical fine, sandlike mottling in the lungs. The tangential shadow of the pleura is displayed along the lateral wall of the chest as a dark lucent strip (arrows).
Blunt trauma to pancreas
• Blunt trauma to pancreas is usually caused by compression against the vertebral column; the best and most common example is seat belt compression injuries. Blunt trauma to pancreas is Usually associated with upper abdominal visceral injury.
• Graded from minor contusion and capsular haematoma (grade I) to severe devascularising crush injury (grade IV).
• Pancreatic trauma is usually damage occurs at most vulnerable segment of pancreas: the junction of the body and tail.
•Laceration–area of intrapancreatic low attenuation, often difficult to see.
•Direct evidence of haemorrhage – fluid around superior mesenteric artery and pancreas.
•Indirect evidence – thickening of anterior pararenal fascia.
- Often requires delayed scans to exclude/monitor complications of pancreatitis and devascularised pancreas.
• Pancreatic abscess.
• Pancreatic pseudocyst.

• Graded from minor contusion and capsular haematoma (grade I) to severe devascularising crush injury (grade IV).
• Pancreatic trauma is usually damage occurs at most vulnerable segment of pancreas: the junction of the body and tail.
Radiological features
- CECT:•Laceration–area of intrapancreatic low attenuation, often difficult to see.
•Direct evidence of haemorrhage – fluid around superior mesenteric artery and pancreas.
•Indirect evidence – thickening of anterior pararenal fascia.
- Often requires delayed scans to exclude/monitor complications of pancreatitis and devascularised pancreas.
Complications of Blunt trauma to pancreas
• Post-traumatic pancreatitis, with:- peripancreatic fat stranding
- diffuse or focal pancreatic enlargement
- irregular pancreatic contour.
• Pancreatic abscess.
• Pancreatic pseudocyst.

Pancreatic trauma. Laceration of the pancreas within the proximal body (arrow heads).
Radiographic anatomy of Paediatric Shoulder
This page contains normal radiographic anatomy of the paediatric shoulder
Images on this page :
* AP
* Lateral
* SI



Source :www.wikiradiography.com
Images on this page :
* AP
* Lateral
* SI
Paediatric Shoulder - AP

Paediatric Shoulder - Lateral

Paediatric Shoulder - Superiorinferior view (SI)

Source :www.wikiradiography.com
Free floating particles in Liqor amnii


Breast Biopsy Spirotome procedure under Ultrasound Guidance
Macrobiopsy of breast lesions is a complicated procedure when performed with vacuum assisted biopsy tools. The Spirotome is a hand-held needle set that doesn’t need capital investment, is ready to use and provides tissue samples of high quality in substantial amounts. In this way quantitative molecular biology is possible with one tissue sample. The Coramate is an automated version of this direct and frontal technology.
Mammographic Findings of Breast Cancer
Findings of mammography in Breast Cancer include :
-High density, speculated mass
-Clustered micro calcifications with variable shape and size; Granular, bizarre micro calcifications are suspicious.
-Well-defined solid masses are sometimes malignant. (Ultrasound is used to determine whether such a mass is solid or cystic).
skin thickening
nipple retraction
focally dilated duct
 # This mammography shows prebiopsy craniocaudal mammogram demonstrates a 1-cm mass in the medial aspect of the breast (see red arrow). Subsequent stereotactic biopsy was performed.
# This mammography shows prebiopsy craniocaudal mammogram demonstrates a 1-cm mass in the medial aspect of the breast (see red arrow). Subsequent stereotactic biopsy was performed.
If mammography detects a non-palpable but suspicious-appearing lesion, needle localization and excisional biopsy or steriotaxic (computer guided) core biopsy can be used to sample the suspicious area. Most mammographers seek a 20-30% positive rate for biopsies of mammographically demonstrated abnormalities.
-High density, speculated mass
-Clustered micro calcifications with variable shape and size; Granular, bizarre micro calcifications are suspicious.
-Well-defined solid masses are sometimes malignant. (Ultrasound is used to determine whether such a mass is solid or cystic).
Secondary Signs of Malignancy
architectural distortionskin thickening
nipple retraction
focally dilated duct

If mammography detects a non-palpable but suspicious-appearing lesion, needle localization and excisional biopsy or steriotaxic (computer guided) core biopsy can be used to sample the suspicious area. Most mammographers seek a 20-30% positive rate for biopsies of mammographically demonstrated abnormalities.
Ultrasound images of Nephrocalcinosis in neonates


Such nephrocalcinosis in neonates usually follows long term parenteral therapy or due to use of certain drugs notably gentamicin and furosemide "furosemide predispose to nephrocalcinosis by increasing urinary calcium excretion. This effect is mediated by inhibition of sodium chloride reabsorption in the thick ascending limb; this is associated with a decline in calcium reabsorption, as calcium transport passively follows that of sodium in this segment.".
Nephrocalcinosis can also be caused by low fluid intake in the neonate and due to oxygen dependency. This condition, in neonates, usually resolves following correction of the etiological factors.
Fibrous cortical defect
Fibrous cortical defect described on X-ray as Small, often multilocular, eccentric lucency that causes cortical thinning and expansion and is sharply demarcated by a thin, scalloped rim of sclerosis. Initially round, the defect soon becomes oval with its long axis parallel to that of the host bone.
NOTES:
Fibrous cortical defect is not a true neoplasm, but rather a benign and asymptomatic small focus of cellular fibrous tissue causing an osteolytic lesion in the metaphyseal cortex of a long bone (most frequently the distal femur). One or more fibrous cortical defects develop in up to 40% of all healthy children. Most regress spontaneously and disappear by the time of epiphyseal closure. A persistent and growing lesion is termed nonossifying fibroma .
Fibrous cortical defect: Multilocular, eccentric lucency in the distal tibia. Note the thin, scalloped rim of sclerosis.
Hyperechoic amniotic fluid


These ultrasound images reveal markedly echogenic (hyperechoic) amniotic fluid. The fluid shows almost the same echogenicity as the placenta. Such appearances of the liquor amni on sonography are seen due presence of vernix caseosa (commonest cause), blood or meconium in the amniotic fluid.
Pneumonia in the Right middle lobe
The right middle lobe is bordered superiorly by the horizontal fissure, and medially by the right heart border. Any abnormality, which increases density of this lobe, may therefore obscure the right heart border, or be limited superiorly by the horizontal fissure.
This x-ray of Child with a cough and fever shows right middle lobe consolidation :
 * The right heart border (right atrial edge) is obscured
* The right heart border (right atrial edge) is obscured
* Consolidation is limited above by a crisp line, formed by the horizontal fissure "red arrow"
* The pathology must therefore involve the right middle lobe
* More extensive shadowing also involves the right and left peri-hilar regions
Diagnosis
* Pneumonia involving the right middle lobe
This x-ray of Child with a cough and fever shows right middle lobe consolidation :

* Consolidation is limited above by a crisp line, formed by the horizontal fissure "red arrow"
* The pathology must therefore involve the right middle lobe
* More extensive shadowing also involves the right and left peri-hilar regions
Diagnosis
* Pneumonia involving the right middle lobe
Subchorionic cyst lesion of the placenta


It may be called:
subchorionic cyst of the placenta Or membranous cyst Or chorionic cyst.It is believed to be due to deposition of fibrin in the subchorionic region of the placenta.
CT scan of Blunt trauma to the spleen
• Spleen is the most commonly injured solid intra-abdominal organ and the Blunt trauma is the most common cause.
• Often (40%) associated with lower rib fractures and left renal injury.
• In 20% of patients with left rib fractures, there is a concomitant splenic injury.
• 25% of patients with left renal injuries also have splenic injuries.
• Damage ranges from subcapsular haematoma to total splenic laceration, potentially leading to exsanguination.


• Often (40%) associated with lower rib fractures and left renal injury.
• In 20% of patients with left rib fractures, there is a concomitant splenic injury.
• 25% of patients with left renal injuries also have splenic injuries.
• Damage ranges from subcapsular haematoma to total splenic laceration, potentially leading to exsanguination.

Rupture of the spleen. This CT shows Rupture of the anterior half of the spleen caused by blunt trauma in falling from a horse.Haemorrhage is seen within the splenic bed (arrow) along with free blood around the liver (arrowhead).

Splenic laceration (arrow).
Appearance of Hydronephrosis in ultrasound
Hydronephrosis refers to a kidney with a dilated pelvis and collecting system. It can be caused by obstruction of the ureters or bladder outlet. Hydronephrosis can also result from reflux (retrograde leakage of urine from the bladder up the ureters to the renal pelvis. Rarely, some children have hydronephrosis without either obstruction or reflux. This is thought to result form abnormal smooth muscles of the renal pelvis or ureter causing ectasia.
 This ultrasound image demonstrates dilated renal calyces indicative of hydronephrosis. Chronic reflux uropathy can lead to hydronephrosis which can result in renal dysfunction as the calyces dilate and compress the renal parenchyma.
This ultrasound image demonstrates dilated renal calyces indicative of hydronephrosis. Chronic reflux uropathy can lead to hydronephrosis which can result in renal dysfunction as the calyces dilate and compress the renal parenchyma.
*Black arrow = renal capsule
*Black arrowhead = sinus fat
*White arrow = dilated calyx
*White arrowhead = renal cortex
 This longitudinal ultrasound shows a kidney with moderate hydronephrosis. The parenchyma is relatively normal in thickness. The dilation of the collecting system extends from the renal pelvis to the calyces. This is a grade III hydronephrosis.
This longitudinal ultrasound shows a kidney with moderate hydronephrosis. The parenchyma is relatively normal in thickness. The dilation of the collecting system extends from the renal pelvis to the calyces. This is a grade III hydronephrosis.

*Black arrow = renal capsule
*Black arrowhead = sinus fat
*White arrow = dilated calyx
*White arrowhead = renal cortex

Ultrasound advantage in Renal calculi investigations
Renal calculi are commonly arise within the collecting renal system. Plain radiographs and intravenous urography are the traditional investigations for renal colic. Ultrasound has the advantage of demonstrating non-opaque calculi and hydronephrosis in comparison with the plain radiographs. Ultrasound has the potential of early diagnosis as compared with intravenous urography.
 Most renal calculi (about 80%) are calcified. Sonographically, stones usually appear as a hyperechoic foci with distal acoustic shadowing . Gas may cause a similar appearance but may have a "dirty" shadow that is not as sharply defined as would occur with a calculus. There may be associated mucosal edema if the stone is impacted or if there is secondary inflammation or infection.
Most renal calculi (about 80%) are calcified. Sonographically, stones usually appear as a hyperechoic foci with distal acoustic shadowing . Gas may cause a similar appearance but may have a "dirty" shadow that is not as sharply defined as would occur with a calculus. There may be associated mucosal edema if the stone is impacted or if there is secondary inflammation or infection.
Hydronephrosis and hydrourether may also be present. Tiny calculi may not cause distal shadowing if they are smaller than the focal zone of the transducer. When there is no shadowing, it may be difficult to distinguish small calculi from echogenic foci caused by fat or other echogenic reflectors within the renal sinus.
Staghorn calculi often appear as multiple, disconnected calculi within the collecting system . Sonography generally underestimates the extent and size of stones in patients with staghorn and other large calculi. The presence of staghorn calculi may make it difficult to diagnose underlying hydronephrosis, because of strong acoustic shadowing from calculi.
Appearance of Renal stones by Ultrasound :

Hydronephrosis and hydrourether may also be present. Tiny calculi may not cause distal shadowing if they are smaller than the focal zone of the transducer. When there is no shadowing, it may be difficult to distinguish small calculi from echogenic foci caused by fat or other echogenic reflectors within the renal sinus.
 |
| Staghorn calculi |
Vertebral artery aneurysm
This Vertebral artery aneurysm or tortuosity causes enlarged cervical intervertebral foramen.
Erosion is caused by pulsatile flow as the vertebral artery passes through the foramina transversaria of the upper six cervical vertebrae between its origin from the subclavian artery and its entrance into the cranial vault through the foramen magnum.


Erosion is caused by pulsatile flow as the vertebral artery passes through the foramina transversaria of the upper six cervical vertebrae between its origin from the subclavian artery and its entrance into the cranial vault through the foramen magnum.


Tortuous vertebral artery. (A) Frontal tomogram shows the enlarged foramen (arrows). (B) Arteriogram shows the tortuous vertebral artery (arrow) entering the enlarged foramen.
Optic nerve glioma; the most common cause of optic nerve thickening

Optic nerve glioma appears as diffuse enlargement of the left optic nerve (arrows) in an 8-year-old girl.
Optic nerve glioma is the most common cause of optic nerve enlargement. Typically causes uniform thickening of the nerve with mild undulation or lobulation. In children (especially preadolescent girls), optic nerve gliomas are usually hamartomas that spontaneously stop enlarging and require no treatment. In older patients, however, these gliomas may have a progressive malignant course despite surgical or radiation therapy. Optic nerve gliomas are a common manifestation of neurofibromatosis (typically low-grade lesions that act more like hyperplasia than neoplasms).

Optic nerve glioma. (A) Sagittal and (B) coronal T1-weighted MR scans show involvement of the chiasm and left optic nerve.
Subscribe to:
Posts (Atom)