A 37-year-old man with a history of spina bifida presented with an audible knocking sound coming from his abdomen during ambulation. Fifteen years earlier he had undergone a cystectomy with a continent cutaneous urinary diversion (Indiana pouch) for a neurogenic bladder. He had been poorly compliant with the catheterization and irrigation regimen involving the pouch.
Physical examination
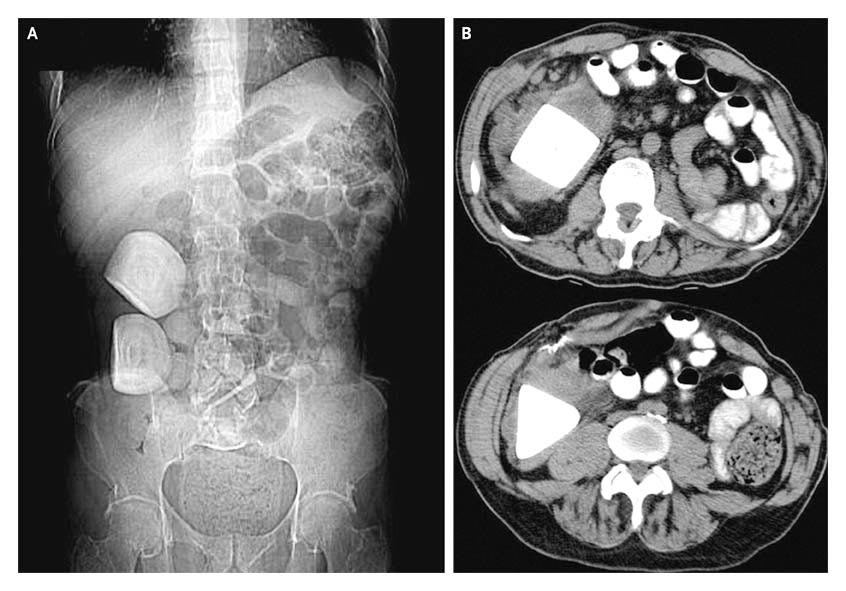
Plain abdominal radiography
Continent urinary diversions may be associated with hypercalciuria, hyperphosphaturia, hyperoxaluria, and hypocitraturia, all of which may predispose patients to pouch urolithiasis. Infections with organisms that break down urea can result in an alkaline environment, which can in turn give rise to struvite (magnesium ammonium phosphate) stones. Establishment of a formal catheterization and irrigation protocol for continent urinary diversions may reduce the risk of urolithiasis.